Oligodendroglioma is a primary braintumor growing in the brain that belongs to gliomas, or supportive tissue tumors. In the following, we will tell you about its prevalence and characteristics.
Oligodendroglioma is one of gliomas
Oligodendroglioma originates and starts to grow from and in brain tissue. It is therefore called a primary brain tumor. (in Latin Primus = first; here primary means what has grown in the brain from the beginning). The brain is located in the head, behind the eyes and forehead. Oligodendroglioma is restricted to the central nervous tissue, usually never outside. It can but rarely does grow in the spinal cord, which also is part of the central nervous system and is attached to the underside of the brain.
Oligodendroglioma is one of the brain tumors called glioma, or supportive tissue or neuroglial tissue tumors. Glioma cells usually resemble a neuroglial cell (glia in Greek =glue) of the brain. Neuroglia surrounds nerve cells and blood vessels meaning they support and service the nerve cells. Oligodendroglioma tumor cells resemble oligodendrocytes, important group cells of the neuroglia.
There are also other supportive cells in the brain, such as astrocytes. In addition to supportive cells, the brain consists of nerve cells and blood vessels and blood cells. Oligodendrocyte cells e.g. form the white myelin around nerve cells which functions as an “insulator”. Their name comes from the Greek words oligos = sparse; dendron = tree and kytos = cell) For more details on the different cells in brain tissue, see Figure ODG 1En
How many oligodendroglioma patients are there?
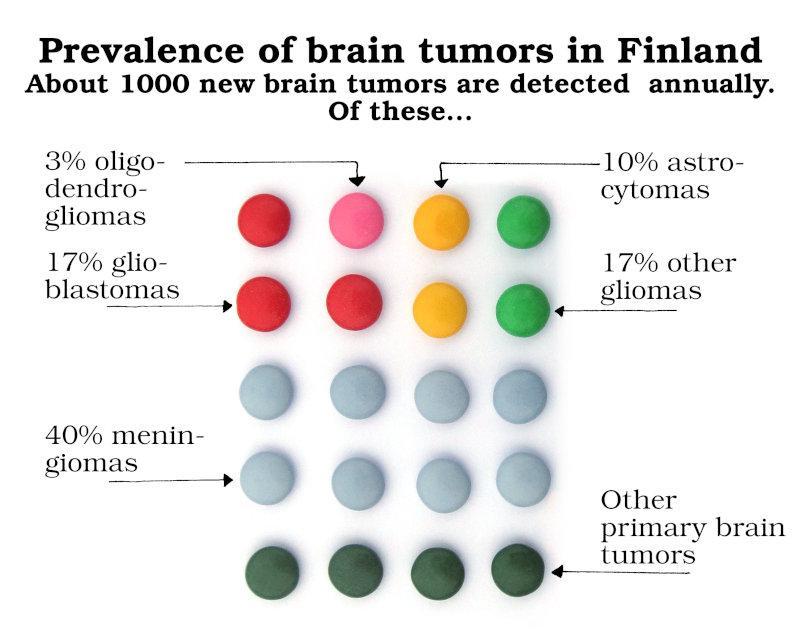
Slightly less than a half of primary brain tumors are gliomas. Less than 10% of all gliomas are oligodendrogliomas. In Finland, over 1000 brain tumors are detected each year, in Sweden about 1400. In Finland, about 30-40 of these brain tumors are oligodendrogliomas. Most oligodendrogliomas occur in middle-aged adults between 40 to 50 years of age. There are currently about 400 people in Finland who have or have had oligodendroglioma. A rough estimate assuming a similar number of oligodendrogliomas would give a 30 000-40 000 people in the Western world having or having had an oligodendroglioma. Probably the real number is even higher.
Where in the brain does oligodendroglioma grow?
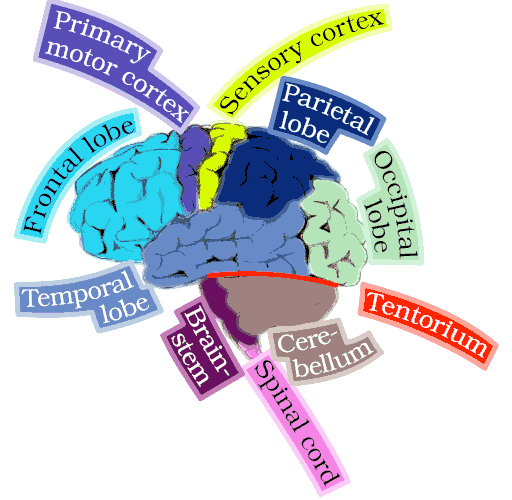
Oligodendrogliomas grow in all parts of the brain. More than 90% of oligodendrogliomas grow, however, in different parts of the cerebral cortex i.e the outer layer of the brain. This area is located in the upper part of the brain, above the tentorium or cerebellum tent. The forehead and temporal lobe are the most common sites for oligodendroglioma. See FIG ODG 3 of different parts of the brain.
Cause and origin of oligodendroglioma
The cause for many tumors is unknown. This is so also with oligodendroglioma. It is not known why they start growing. It was previously thought that oligodendrogliomas begin to grow from brain supporting i.e glial cells called oligodendrocytes (oligodendro = few: protrusions). Recent research has shown that the onset of oligodendroglioma is more complex and involves brain cells in the stem cell state. Then there become mutations in these cells. Mutations mean abnormal changes and damages in the genetic material, genes and particularly their DNA. After sufficient number and kind of mutations accumulate an oligodendroglioma starts growing. Whether the tumor becomes oligodendroglioma or some other glioma, such as astrocytoma, depends on these genetic modifications in the cell that is these mutations.
It is not known whether some people produce more of these mutations or whether their bodies destroy them less. It is suspected that some people have such resistance mechanisms that their body destroys the transformed cells early. In others, the body does not destroy these mutated cells as easily. The growth pattern of gliomas is poorly understood and cannot be influenced.
Characteristics of oligodendroglioma
General Oligodendrogliomas are usually soft, gray tumors. They often contain calcifications, bleeding and / or cysts (cyst= a pouchlike, often tiny structure). In appearance they do not differ very much from the normal brain. Oligodendrogliomas are made up of many kinds of cells. They do not contain a single type of cell. Thus, the different spots in the tumor are somewhat different. This property, which is typical of all gliomas, including oligodendrogliomas, is called heterogeneity, i.e. mixed composition or inhomogeneity. This should be recognized, as tumor heterogeneity is important to take into consideration both for determining what kind of tumor it is and for treatments and treatment outcomes.
The sample of the tumor taken in the operation or biopsy is what is being examined. The tumor is practically never completely removed. So it must be remembered that we do not know exactly what kind of tumor cells were left in the brain. Under the following subheadings, I will also discuss what this means in practice.
Tumor cells
The diameter of one tumor cell is about 20 μm, so 50 tumor cells fit in a line one millimeter long and almost 1300 in a line one inch long. The cells are viewed under a microscope usually with several hundred times magnification.
If an oligodendroglioma cell is magnified 400 times it looks 8 mm(1/3 of an inch) in diameter. Under a microscope, tumor cells look like having “short hands” and like a fried egg. Not all cells in the tumor look the same some may have the appearance of an astrocyte, which is another type of glial cell. Thus, different parts of the tumor may look different. In magnetic resonance imaging (MRI), the boundary to the normal brain can appear sharp. However, this is not really the case in the brain, for the margin to the normal brain is diffuse. Normal brain cells can grow inside the tumor, and there may be tumor cells in the adjacent brain tissue that looks normal, see Figure ODG 4En.
The basis for oligodendroglioma diagnosis
The diagnosis of oligodendroglioma is always based on the pathologist’s report after examining a sample of the tumor. One cannot make a definitive diagnosis of tumor type on the basis of MRI scans only. The pathologist describes the microscopic appearance of the tumor as well as the number of cells that are in the dividing stage, which tells about the malignancy. In addition, chromosomes and certain genetic defects from the genome of the tumor cells are determined. ). It is worth remembering that the report is based on the piece of tissue available to the pathologist. The excised tissue is not always exactly the same as the part left in the brain.
How malignant is oligodendroglioma?
Brain tumors are classified according to the most malignant part of the sample the pathologist gets to analyze. Oligodendrogliomas are class II or III in malignancy, the higher the number, the more malignant.
Class IV tumors are no longer called oligodendroglioma but glioblastoma. If glioblastoma has cells that look like oligoden droglioma, it is still called glioblastoma according to the current classification.
There is no class I oligodendroglioma, although some class II oligodendrogliomas are so slow-growing that they almost meet the class I criterion.
Because the tumor is classified according to the most malignant part, the heterogeneity of the oligodendrogliomas may affect the outcome. It may be that the most malignant part has been operated and is being examined by a pathologist, leaving the slower-growing cells in the brain. Conversely, it may be that the part operated and the pathologist gets to analyze is a more benign i.e. slower growing part and the more malignant cells remain in the brain.
Chromosomal changes
An essential feature of oligodendroglioma is the changes in chromosomes 1 and 19. Chromosome 1 lacks the second short arm (p) and chromosome 19 the other long arm (q). Usually this is called 1p19q deletion. Today, these chromosomal changes are a prerequisite for oligodendroglioma diagnosis. If the tumor looks microscopically like oligodendroglioma, diagnosis cannot be made unless there is this 1p19q deletion. On the other hand, even if many cells in the tumor look like astrocytes, if the 1p19q deletion is present, the tumor is an oligodendroglioma.
Genetic changes
Some genes are also tested in addition to the chromosomes. The genes that regulate the IDH1 or 2 enzyme are significant. Do these genes have a mutation? These enzymes are important for the cell’s energy metabolism. If IDH 1 and sometimes IDH2 mutations are detected, the tumor often has a better prognosis. In oligodendroglioma IDH1 and 2 are rarely intact that is unmutated. A typical oligodendroglioma is a grade II tumor which has IDH1 and/or 2 mutation and 1p19q deletion.
The significance and utilization of the mutations in the therapy of the tumors are at an early stage, but research is intense. Other genetic changes can also be described in a pathology report. The appearance of the tumor sample can also be described in more detail. Often it is reported which proportion of the cells appear to be dividing telling the. Ki-67 percent. Usually it is low in grade II oligodendroglioma, often below 10%.